

What is a chest wall deformity?
A chest wall deformity is a condition where the shape of the chest develops abnormally. It can be noticed at birth, but more likely becomes more evident as your child goes through a growth spurt. This can range from very mild to severe. It happens when the cartilage that connects the ribs grows unevenly. Doctors aren’t sure why this occurs, but it often runs in families and may be associated with growth patterns during adolescence.The two most common types:

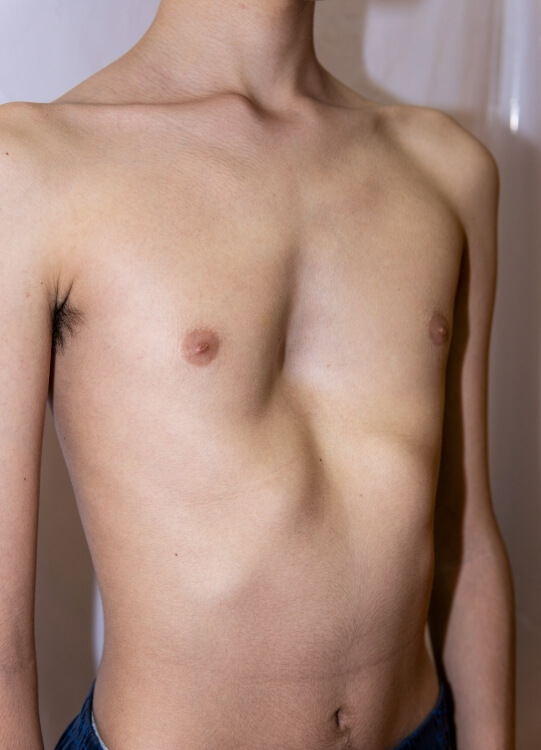
Pectus excavatum (funnel chest)
In this condition, the breastbone (sternum) curves inward, making the chest look sunken. It’s the most common type of chest wall deformity, affecting about 1 in every 300–400 children. Boys are more likely to have this condition than girls.
In this condition, the breastbone (sternum) curves inward, making the chest look sunken. It’s the most common type of chest wall deformity, affecting about 1 in every 300–400 children. Boys are more likely to have this condition than girls.
Pectus carinatum (pigeon chest)
Here, the breastbone and ribs stick outward. Sometimes both sides of the chest protrude, and other times one side sticks out more than the other. This type affects about 1 in every 1,500 children and is also more common in boys.
Here, the breastbone and ribs stick outward. Sometimes both sides of the chest protrude, and other times one side sticks out more than the other. This type affects about 1 in every 1,500 children and is also more common in boys.
We can also treat other chest wall conditions like slipping rib syndrome (SRS), a condition where the lower ribs become hypermobile, slipping out of place and causing sharp pain in the lower chest. Dr. Rader also treats Poland syndrome.
Signs & Symptoms of a Chest Wall Deformity in Children and Teens
Some chest wall deformities are mild and do not result in symptoms. Other children may have stamina problems or breathing problems, particularly during physical exercise or sports. Sometimes, irregular heartbeats or abnormal EKG readings can be noted by the patient’s physician.
Children with more pronounced chest wall deformities may feel very self-conscious about their appearance and avoid activities like swimming, where their chests are exposed.
Our Approach to Treatment
At Stamford Health, Dr. Christine Rader is experienced in the Nuss procedure to address chest wall deformities. This surgery is recommended for patients beginning at age 14, but evaluations for chest wall deformities are done at any age.
Nuss Surgery for Pectus Excavatum: What To Expect
- A pediatrician or primary care physician will need to refer the patient to Dr. Rader.
- During an initial consultation, Dr. Rader will evaluate the patient, order necessary imaging studies and discuss the options, including surgery. She will answer all questions about what a patient can expect.
- Next, the patient will need to have a chest X-ray or a CT scan to evaluate the severity of the chest wall deformity and may need a fitness test. One commonly used measurement is the Haller Index, which helps guide treatment decisions. All these tests can be done with Stamford Health’s imaging centers located throughout Fairfield County.
- If the patient is determined to be a good candidate for the procedure, it will be scheduled and performed at Stamford Hospital. The typical patient will go home in one or two days.
- During the surgery, a metal bar shaped to fit the patient is placed in the pathway under the sternum and then rotated to lift the chest and correct the deformity. After 2-3 years, the bar is removed during an outpatient surgery.
Patient Stories
Meet Dr. Christine Rader, Director of Pediatric Surgery

Dr. Rader grew up in Brookfield, Connecticut, and attended college and medical school in Boston. She completed her general surgical training at the University of Connecticut, and then her specialized training in pediatric surgery at Yale University.
Most recently, Dr. Rader worked at Connecticut Children’s Medical Center performing all aspects of pediatric and neonatal surgery. Here, she developed an interest in patients with pectus excavatum. As she began to treat these patients, she realized that she can make a difference in their lives by intervening at a time when self-confidence can be hampered by body image and physical limitations.
Having the surgery to fix pectus excavatum is a big decision for families, but the majority of patients do not regret it. This often gives kids a new lease on life and is a very positive experience for them. Dr. Rader is happy to support families throughout the process.
Meet Dr. Christine Rader, Director of Pediatric Surgery
Dr. Rader grew up in Brookfield, Connecticut, and attended college and medical school in Boston. She completed her general surgical training at the University of Connecticut, and then her specialized training in pediatric surgery at Yale University.Most recently, Dr. Rader worked at Connecticut Children’s Medical Center performing all aspects of pediatric and neonatal surgery. Here, she developed an interest in patients with pectus excavatum. As she began to treat these patients, she realized that she can make a difference in their lives by intervening at a time when self-confidence can be hampered by body image and physical limitations.
Having the surgery to fix pectus excavatum is a big decision for families, but the majority of patients do not regret it. This often gives kids a new lease on life and is a very positive experience for them. Dr. Rader is happy to support families throughout the process.
FAQs About Pectus Excavatum & Chest Wall Deformities
-
How do you know if you require surgery for pectus excavatum?While the dip in the sternum may be obvious on the outside of the body, some measurements done with the aid of X-rays or CT scans provide information about the severity of the problem. One commonly used measurement is the Haller Index, which helps doctors assess the degree of chest wall compression. A mild deformity may not necessitate surgery. In addition, we discuss symptoms, including self-esteem and physical activity.
-
Is the Nuss Procedure or the “MIRPE” a painful procedure and how is the pain managed?The immediate result of pushing out the sternum with a chest prosthetic can be quite painful, however, as with most centers around the country, Dr. Rader uses “cryoablation.” This is a technique of freezing the nerves of the chest wall to numb the chest after surgery. With the addition of this technique, patients can typically go home the next day after surgery.
-
How long is the recovery period after pectus excavatum surgery?The initial recovery is about 1-2 weeks, but it takes a month or two to adjust to a different posture and chest alignment. However, returning to work or school is acceptable after 1-2 weeks. Returning to organized sports or contact sports typically occurs after 3 months.
-
How long does the implant stay in the patient?The implant stays in for at least 3 years. The surgery to remove the implant is outpatient surgery, with patients going home the same day.
-
Are there any non-surgical treatment options for pectus excavatum?The is currently something called the “vacuum bell” which is a suction cup device applied to the chest wall to help correct pectus excavatum. Dr. Rader can discuss this therapy with patients and their families.